Early observational studies described some degree of cardiac involvement in up to 78% of infected Covid-19 patients, ranging from troponin elevations to features of myocarditis and myopericarditis on cardiac magnetic resonance imaging (CMR).
Therefore the uncertain risks for myocarditis, a leading cause of sports-related sudden cardiac death, should be factored when considering return to play for athletes after Covid-19 with and without symptoms.
What does the data currently tell us?
In October 2020, Kim and colleagues, representing the American College of Cardiology’s Sports and Exercise Council, published recommendations for the evaluation of athletes who had tested positive for COVID-19 to ensure safe return to play.
The group recommended a tiered approach based on:
- The presence of symptoms, followed by
- Electrocardiography (ECG),
- Injury biomarkers (troponin), and
- Echocardiography
Abnormalities were then to be further characterized by the selective use of cardiac magnetic resonance imaging. The recommendations were based on expert opinion of experienced sports cardiologists, because there were at the time only limited data to inform such a document.
Moving on since then, there has been a remarkable amount of information acquired, analyzed, and published regarding post–COVID-19 prevalence of cardiac abnormalities in athletes.
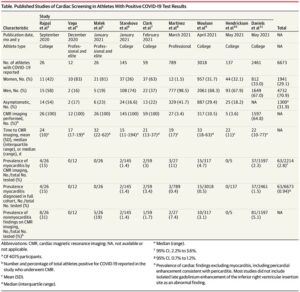
Starting in September 2020, the Big Ten athletic conference (involving 13 major universities) mandated comprehensive cardiac screening, including ECG, troponin testing, echocardiography, and CMR imaging for athletes in the aftermath of positive COVID-19 test results, regardless of prior symptomatic status.
The authors report on a large sample of 2461 athletes, they found that 37 of these athletes met the diagnostic criteria for myocarditis by CMR imaging, 20 without cardiovascular symptoms and with normal ECG, echocardiography, and troponin test results, who would not have been identified without the CMR imaging.
Screening only on the basis of COVID-19 symptoms is not reliable. Sensitivity is improved by combining the presence of symptoms as well as ECG, echocardiography, and troponin testing results. Further, this approach will likely miss individuals who appear normal with CMR imaging evidence of myocarditis.
What are the implications of finding evidence on CMR imaging of myocarditis in the absence of prior symptoms or abnormalities on cardiac testing?
It is unclear if abnormalities on CMR imaging after COVID-19 represent increased risk of sudden death in athletes. This is because myocarditis in athletes in the past has been diagnosed in the presence of cardiovascular symptoms and not by screening asymptomatic individuals with CMR imaging.
On the other hand, the absence of symptoms in athletes with myocarditis does not mean lesser risk because in an autopsy series of proven myocarditis, more than 50% of athletes were asymptomatic prior to death.
Does this suggest that CMR imaging should be the primary screening modality?
The practicality (cost and access) when applied to most populations is challenging as it would place a major burden on any health care system.
The more practical and more widely available approach would be of testing with ECG, echocardiography, and serum troponin in the following manner:
1. The presence of moderate to severe symptoms with initial COVID-19, or persistent or recurrent symptoms, would require initial cardiac evaluation with ECG, serum troponin, and echocardiogram.
2. Cardiac MRI is recommended for athletes with abnormalities on these initial cardiac screening tests.
What is still unknown?
Low risk athletes: those without abnormal cardiac screening tests and without moderate symptoms (eg, dyspnea, chest pain, lethargy, hypoxia)—the clinical significance of abnormal MRI findings suggestive of injury and inflammation is yet unknown and needs to be interpreted cautiously.
The potential risks and screening protocols need to be discussed with athletes, their families, coaches, trainers, sports scientists, and doctors. An evaluation strategy with the medical team will help identify many potential cases of cardiac involvement.
This article specifically focusses on the athlete’s heart. Other standard screening tests must be performed in consultation with the athlete’s treating doctor to obtain a clearance for return to play. This will most certainly ensure safe return to play for athletes with a history of Covid-19.
~ Authored by Yash Chhatbar Sport Physiotherapist, Mind Your Fitness!